A milestone in DRC’s campaign to make vaccination planning more effective and equitable
The GRID3 Mapping for Health project (GRID3 M4H) has reached a major milestone in its 19-month effort to support vaccination interventions in the Democratic Republic of the Congo (DRC). Funded by Gavi’s INFUSE programme, the project’s primary aims were to bolster routine immunisation via the generation of core spatial data (on population, boundaries, health facilities, and settlements), support geo-enabled microplanning, generate mobility data that would support regular updating of resources needed for routine childhood immunisation nationwide (such as restocking vaccine supplies or boosting the number of health staff in a facility), enable health planners to strengthen their geospatial analytical skills, and improve the gender equity of routine childhood immunisation and vaccination intervention planning.
The project is an initiative of DRC’s ministry of health (Ministère de la Santé) and relied on the expertise of a wide array of organisations, both governmental and non-governmental. The work was led by the Center for International Earth Science and Information Network (CIESIN) and the Flowminder Foundation, and supported by WorldPop. At the national level, key collaborators were the Expanded Programme on Immunisation (EPI), Acasus, UNICEF, WHO, UNOPS, and the Kinshasa School of Public Health (KSPH).
GRID3 M4H was conceived to directly support the realisation of the Mashako Plan, an effort to boost vaccine coverage in targeted provinces and protect 220,000 additional children nationally through more effective and equitable vaccination interventions.
Upon the project’s commencement in June 2020, GRID3 M4H first focused on facilitating strong multi-stakeholder engagement. A steering committee and a technical committee were formed to guide implementation; by soliciting the input and guidance of DRC officials, the committees ensured government ownership of the effort and supported sustainability, as well as provided networking opportunities for all participants. With the proper organisational structures in place, the project began its data collection phase.
Having accurate data on the boundaries of health areas and health zones, as well as the locations of health facilities and settlements, is crucial to effective microplanning for vaccination. Accordingly, a major aspect of the project’s data work was producing basemaps and a gridded population layer that would serve as a fundamental component of maps and immunisation plans for each health area.
A massive fieldwork exercise involving 27 GIS technicians/coordinators and over 2,000 people from local health teams was carried out in 5 provinces (Kinshasa, Kasaï, Kasaï Oriental, Haut Katanga, and Lomami) with the purpose of collecting data on health facilities, health catchment areas, settlements, schools, religious centres, and other points of interest for the maps. Additionally, data and maps are being produced for Haut-Lomami, Kwilu, Ituri, and Tanganyika provinces via cleaning and consolidating existing data from partners and previous GRID3 fieldwork. By the end of October 2022, GRID3 will have produced and distributed nearly 4,000 health area and health zone level maps across 9 provinces.
With the DRC’s last census having taken place in 1984, there was an urgent need for accurate and reliable population estimates that can be used to plan health service delivery, including vaccination interventions. To that end, the project produced bottom-up gridded population estimates.
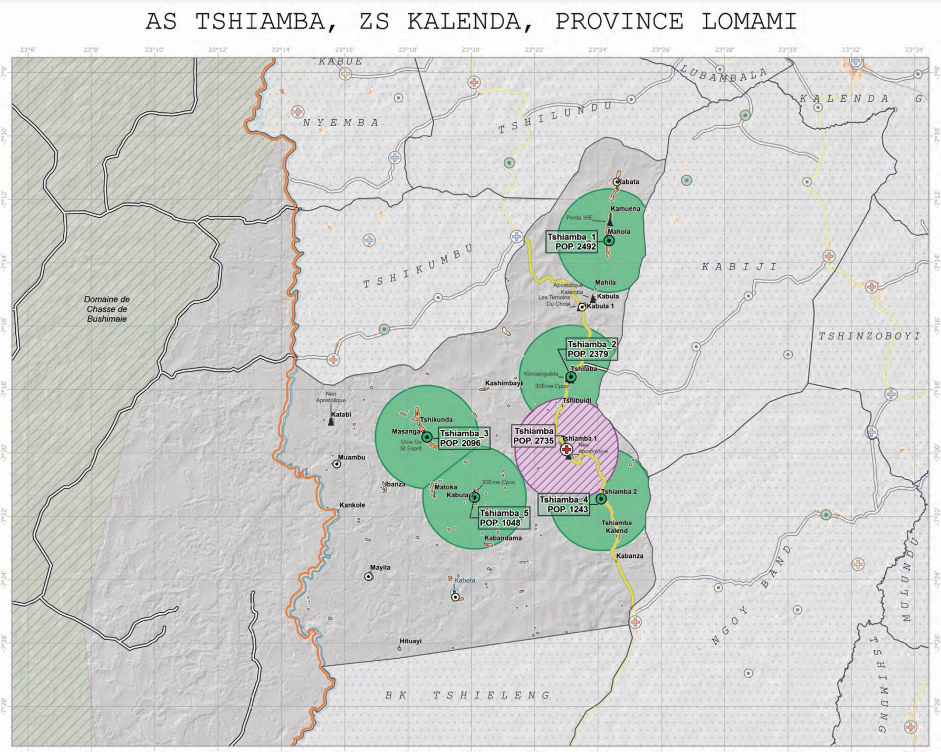
The first stage of creating the estimates was a microcensus survey implemented by KSPH. The microcensus took place between March and April 2021, with enumerators visiting a sample of 1,596 clusters spread across 7 provinces. These survey data were combined with some 500 geospatial covariates to create government-endorsed bottom-up population estimates for Haut-Katanga, Haut-Lomami, Ituri, Kasaï, Kasaï-Oriental, Lomami, and Sud-Kivu. Once produced and validated, the basemaps and high-resolution gridded population estimates data were fed into Flowminder’s optimisation algorithm (which used the data to model optimal locations for vaccination sites) with the target of having nearly 100 percent of the population live within 3km of either a fixed or a mobile vaccination post. The data outputs were combined to produce maps and immunisation plans for each health area. These documents included a summary page with key indicators such as the total and target population of the health area (as well as number of fixed and advanced sessions sites); a microplanning map of the health area containing the fixed and advanced vaccination sites (indicated with colour codes); as well as more-detailed tables breaking down the information for each vaccination site (by minimum frequency, population to be covered, and villages covered).
The project produced the nationwide population mobility estimates using anonymised and aggregated mobile operator data (call detail records, CDRs) and data from the project’s phone survey. The responses from the survey also supported the analysis of the CDR data and improved understanding of how demographics and mobility vary among subscribers of different mobile network operators in the DRC; among subscribers in different regions; and among those who use their phones often versus those who do not. Completed in the first week of November 2021, the survey included respondents from all the country’s provinces and interviewed a total of 7,500 people.
At a project-related event in November 2021, 95 percent of health professionals in attendance indicated they found the mobility data to be useful for their vaccination services, as the indicators can help to provide insights into both gradual population trends and sudden population movements. This echoed feedback the project team received from data managers and health zones’ head doctors (medecins chefs de zones) during the user-consultation sessions held in June 2021.
Currently, outputs from the phone survey and the microcensus survey are being combined with geospatial data to develop a statistical model and produce mobility estimates that are adjusted to reduce representation and measurement biases inherent to working with CDR data. The mobility estimates will be made available to the Ministry of Health staff via DHIS2.
Knowledge sharing and capacity development formed a major component of the project, ensuring meaningful in-country ownership and application of its data.
Capacity strengthening in the use of data products was designed to augment the skills of in-country partners so that they could 1) use geospatial and demographic data using QGIS and 2) make interpretations necessary for health planning and policy making. Concurrently, the project team worked with stakeholders and health workers to identify the most pressing social barriers to increased vaccination coverage in two provinces.
GIS training sessions were delivered to national- and province-level data managers. A total of 54 data managers and info sanitaire (infosan) workers from selected priority provinces were trained in foundational and intermediate GIS over 5 different training sessions. By the end of all the training sessions, participants were able to process and visualise geospatial data using QGIS, as well as produce beginner- and intermediate-level maps on the QGIS software.
Related to the examination of social barriers, the project also produced resources to promote and help improve gender equity in immunisation services. A gender equality and social inclusion (GESI) audit took place in four health zones in Kasaï and Kinshasa; the audit consisted of interviews, questionnaires, and a literature review that provided the opportunity for an in-depth assessment of the gender equity of vaccination interventions. The results informed the production of a Gender Based Analysis Barrier and Action Planning (GBA+) toolkit, a multi-purpose resource consisting of a training curriculum and two manuals on integrating gender-based and social inclusion analysis in vaccination programmes. The kit’s various tools have been carefully designed to encourage and support vaccination actors to mainstream gender equity considerations into their programme’s design, implementation, and monitoring and evaluation.
Gender and social inclusion training was enacted via a “training of trainers” (ToT) approach. Overall, three ToT sessions trained 51 health and social care professionals (referred to as “ambassadors”) on gender and social inclusion in vaccination interventions across 2 health zones in Kinshasa, 3 health zones in Kasaï, and 8 organisations across both provinces. In turn, 25 gender equity sensitisation sessions conducted by those ambassadors trained a total of 311 healthcare practitioners in Kinshasa and Kasaï.
The achievements of the GRID3 M4H project are considerable. The population estimates, basemap data, and modelled locations for fixed and advanced vaccination sites were combined to create maps and geo-referenced microplanning support documents that are all in the process of being printed and shipped to the relevant health zones.
Meanwhile, the microcensus data on demography, household composition, mobility, migration, phone use, and other areas will be of immense value to national statisticians, researchers, and other data analysts; the National Statistical Institute has stated its intent to use the population estimates to support its next census mapping exercise, planned for later this year. Overall, the basemaps, gridded population estimates, mobility estimates, gender equality, social inclusion resources, and microplanning support documents have the potential to contribute greatly to enhancing the effectiveness and equity of vaccination interventions and other national programmes.
Just as important, the project’s consistent involvement of stakeholders in every step of the process has paved the way for sustained use of geospatial data in DRC’s routine immunisation campaigns.
Supported by Gavi through its INFUSE initiative, GRID3 Mapping for Health in the Democratic Republic of the Congo (DRC) was a ministry of health initiative delivered in partnership with Flowminder and the Center for International Earth Science Information Network at Columbia University (CIESIN). The project was a continuation of previous work conducted and/or supported in DRC by the GRID3 programme.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}